Diagnostic Criteria for AOM
Diagnosing AOM involves the following:
- Identify the presence of 1 or more of the following:
-
- Moderate to severe bulging of the tympanic membrane
- Mild bulging of the tympanic membrane and recent (<48 hours) onset of ear pain* (Click to review signs of otalgia in a nonverbal child.)
- Intense erythema (redness) of the tympanic membrane
- New onset of otorrhea not due to acute otitis externa
- Assess the severity and laterality of symptoms to determine treatment options.
- Treat in these cases:
- Severe AOM (fever ≥39°C [102.2°F], moderate to severe otalgia, or otalgia for at least 48 hours)
- Bilateral, nonsevere AOM in young children 6–23 months of age
- Otorrhea
- Initial observation (watchful waiting) for 48–72 hours is an option in these cases:
- Nonsevere*, unilateral AOM in young children 6–23 months of age
- Nonsevere*, unilateral or bilateral, AOM in older children ≥24 months of age
*Nonsevere AOM = mild otalgia <48 hours and fever <39°C (102.2°F)
Note: In children with viral disease such as respiratory syncytial virus (RSV), middle ear fluid is common and does not require antibiotic treatment.
When examining the tympanic membrane, consider the following:
- Ensure adequate visualization of the tympanic membrane, which may require cerumen removal.
- Perform tympanic membrane air insufflation to assess mobility (decreased mobility of the tympanic membrane on pneumatic otoscopy indicates middle ear effusion [MEE]).
Figure 2 below from the AAP Clinical Practice Guideline: The diagnosis and management of acute otitis media illustrates differing degrees of TM bulging. You may want to consider making such images available to clinicians in examination rooms.
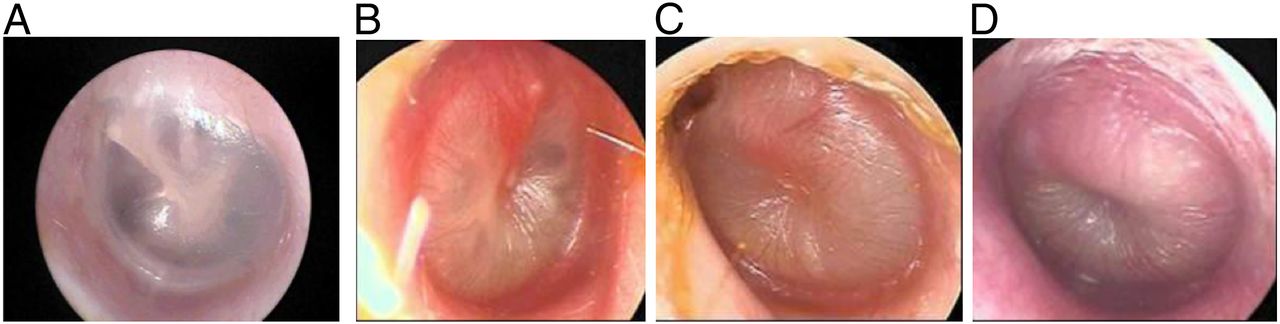
FIGURE 2 shows A Normal TM; B TM with mild bulging; C TM with moderate bulging; D TM with severe bulging.
Image provided courtesy of Alejandro Hoberman, MD.